

Introduction
Urolithiasis has long been a painful companion of humanity, afflicting men more than women, and costing health systems billions annually. Among all urinary tract stones, distal ureteric stones (DUS)—stones lodged in the lower third of the ureter—represent more than 70% of cases. While many stones pass spontaneously, those measuring 5–10 mm often resist conservative measures, leaving patients in agony and physicians in search of better strategies.
Traditionally, treatment options have ranged from watchful waiting and medical expulsive therapy (MET) with alpha-blockers or calcium-channel blockers, to invasive interventions such as extracorporeal shock wave lithotripsy (ESWL) or ureteroscopy. Each option comes with its own baggage: spontaneous passage rates are modest, MET is variably effective, and surgery, though often curative, is costly and not without complications.
Into this landscape enters a most unexpected contender: sildenafil citrate, the world’s most famous phosphodiesterase-5 (PDE5) inhibitor. Known for revolutionizing erectile dysfunction management, sildenafil also exerts smooth muscle relaxant effects via nitric oxide (NO) and cyclic guanosine monophosphate (cGMP) pathways. Could this mechanism be harnessed for the ureter, facilitating stone expulsion and reducing patient suffering?
The randomized controlled trial (RCT) by Shokeir and colleagues (2016) sought to answer precisely this question. The results open intriguing possibilities for broadening sildenafil’s therapeutic portfolio far beyond the bedroom.
The Pathophysiology of Distal Ureteric Stones
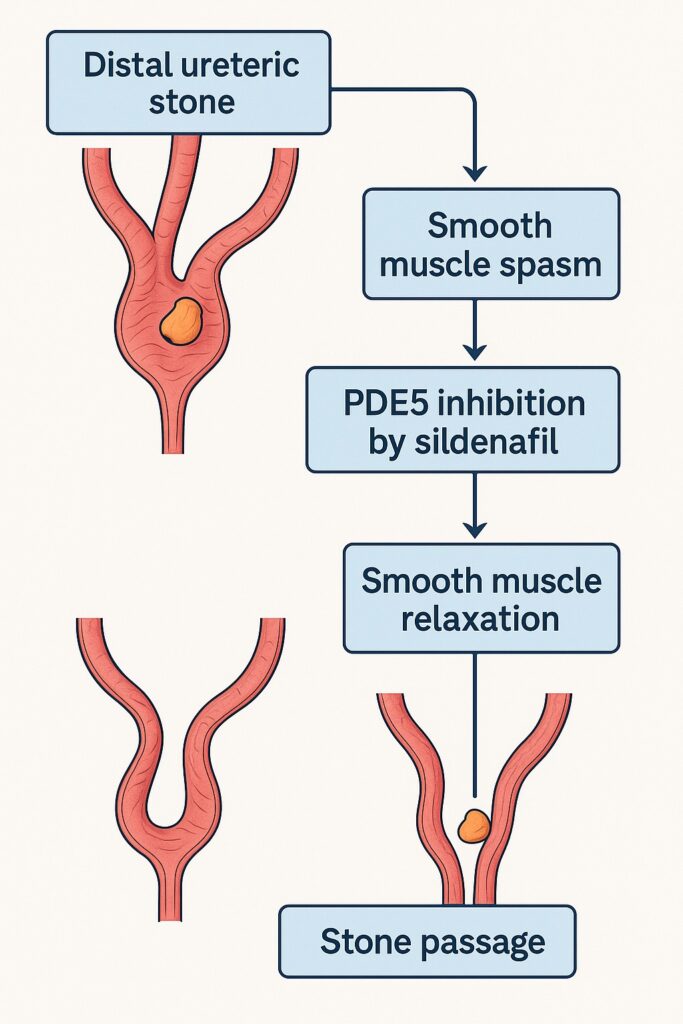
Stones lodge in the distal ureter for both mechanical and physiological reasons. Narrow luminal diameter, increased mucosal folds, and strong ureteric peristalsis all contribute to resistance against downward passage. The irritation from the stone triggers smooth muscle spasm, edema, and local inflammation, further tightening the grip.
Smooth muscle tone in the ureter is controlled by a delicate balance of neurotransmitters—adrenergic, cholinergic, and non-adrenergic non-cholinergic systems—as well as endothelial mediators. At the molecular level, cyclic nucleotides (cAMP and cGMP) are the key messengers orchestrating relaxation and contraction. PDE5 enzymes degrade cGMP, tightening smooth muscle tone. By inhibiting PDE5, sildenafil effectively prolongs cGMP signaling, promoting sustained smooth muscle relaxation.
Thus, from a mechanistic standpoint, sildenafil seems a logical candidate for reducing ureteric spasm and encouraging stone passage.
The Clinical Trial: Design and Execution
The Egyptian trial was a randomized, double-blind, placebo-controlled study—the gold standard in clinical research. Conducted at Mansoura University’s Urology and Nephrology Center, it enrolled 100 men aged 18–65 years with single, unilateral, radiopaque distal ureteric stones measuring 5–10 mm.
Key inclusion criteria ensured homogeneity: normal renal function, absence of infection, and exclusion of high-risk situations such as solitary kidney or bilateral stones. Patients were randomized into two equal groups:
- Sildenafil group: 50 mg sildenafil citrate once daily.
- Placebo group: identical-looking placebo tablet once daily.
Both groups received supportive care, including analgesics when required. Patients were followed for up to four weeks or until stone passage, with interventions (ESWL or ureteroscopy) offered if expulsion failed or complications developed.
Importantly, both patients and investigators were blinded to treatment assignment, eliminating bias.
The Results: Sildenafil Outperforms Placebo
The findings were striking. Spontaneous stone expulsion occurred in 67.3% of patients receiving sildenafil, compared to only 40.4% in the placebo group—a statistically significant difference (P = 0.014).
Equally compelling was the time to stone passage:
- Sildenafil group: average 11.5 days
- Placebo group: average 17.2 days
This nearly one-week acceleration in passage time is clinically meaningful. Faster expulsion translates into fewer days of colic, reduced analgesic use, and less psychological burden for patients.
Multivariable Cox regression confirmed sildenafil as the only independent predictor of successful stone passage, with a hazard ratio of 2.7 (95% CI: 1.5–4.8). In other words, patients were nearly three times more likely to pass their stone when taking sildenafil.
Adverse effects were minimal: only two patients reported headaches, managed with paracetamol. No cases of severe hypotension, arrhythmia, or serious complications were observed.
Mechanistic Insights: Sildenafil vs Traditional MET
Alpha-blockers such as tamsulosin have long been the mainstay of MET. Their mechanism—blocking α1-adrenergic receptors—reduces basal tone in the ureter and bladder neck, facilitating expulsion. Yet their efficacy varies, and not all patients respond.
Sildenafil works differently. By amplifying NO–cGMP signaling, it induces profound smooth muscle relaxation not just in penile tissue but in ureteric walls. This mechanism complements adrenergic blockade and might even surpass it in specific contexts.
Interestingly, the study also highlights an unresolved question: is sildenafil’s benefit solely due to direct ureteric smooth muscle relaxation, or is it partly mediated by increased sexual activity (and thus NO release) among men taking the drug? The trial did not assess sexual frequency, leaving this as a tantalizing research gap.
Comparison with Other Therapies
When placed alongside established therapies, sildenafil emerges as a strong contender:
- Versus placebo: Clearly superior, with higher expulsion rates and faster passage.
- Versus alpha-blockers: Comparable efficacy, though head-to-head trials are lacking. Some pilot studies suggest PDE5 inhibitors may rival or even outperform tamsulosin.
- Versus calcium channel blockers: Likely safer and better tolerated, as calcium blockers often produce hypotension and dizziness.
The possibility of combination therapy—sildenafil plus tamsulosin—remains an exciting frontier. Such dual therapy could theoretically maximize smooth muscle relaxation via complementary pathways, but safety must be carefully evaluated.
Safety and Limitations
The safety profile of sildenafil in this trial was reassuring. No serious adverse effects occurred, and headaches were the only notable complaint. Given sildenafil’s widespread use and well-characterized cardiovascular risks, this finding reinforces confidence in its short-term safety for otherwise healthy men.
Limitations of the study must be acknowledged. The sample size, while adequate for statistical power, remains relatively small. Only men were included, limiting generalizability. The trial also did not monitor sexual activity, an omission that complicates mechanistic interpretation. Finally, the four-week follow-up may not capture long-term recurrence or late complications.
Clinical Implications
For practicing urologists, the take-home message is clear: sildenafil citrate is a safe and effective option for MET in men with 5–10 mm distal ureteric stones.
Its role should not be seen as replacing alpha-blockers, but rather expanding the armamentarium. In men who cannot tolerate tamsulosin (due to hypotension or ejaculatory dysfunction), sildenafil may be a valuable alternative. In men with both ureteric stones and erectile dysfunction—a not uncommon coincidence—it offers dual benefits.
However, caution is warranted in patients on nitrates or with significant cardiovascular comorbidities, where sildenafil remains contraindicated.
Future Directions
The trial opens more doors than it closes. Future research should explore:
- Head-to-head comparisons between sildenafil and alpha-blockers.
- Combination regimens of PDE5 inhibitors and α-blockers.
- Mechanistic studies to disentangle direct smooth muscle effects from sexual activity–mediated pathways.
- Inclusion of women, who are also affected by ureteric stones, albeit at lower rates.
Ultimately, sildenafil may emerge not as a replacement but as part of a tailored, patient-centered approach to stone management.
Conclusion
The use of sildenafil citrate for distal ureteric stones may sound unconventional, but the evidence speaks volumes. This humble PDE5 inhibitor, already a household name for entirely different reasons, demonstrates real potential as a medical expulsive therapy.
By significantly increasing stone passage rates and reducing time to expulsion—with minimal side effects—sildenafil has earned its place at the urologist’s table. Whether it will become standard of care remains to be seen, but one thing is certain: in the story of ureteric stones, sildenafil may yet play an encore role outside its famous stage.
FAQ
1. How does sildenafil help in passing ureteric stones?
Sildenafil inhibits PDE5, which prolongs cGMP activity and enhances smooth muscle relaxation. In the ureter, this relaxation reduces spasm and resistance, facilitating stone expulsion.
2. Is sildenafil more effective than tamsulosin for ureteric stones?
Current evidence suggests comparable efficacy. Sildenafil significantly improves stone expulsion compared with placebo, but head-to-head trials with alpha-blockers are still needed.
3. Can all patients with ureteric stones take sildenafil?
No. It is suitable for otherwise healthy men, particularly with 5–10 mm distal stones. It should not be used in patients taking nitrates or those with severe cardiovascular disease.
