

Introduction
Erectile dysfunction (ED) is not merely an inconvenience of intimacy; it is a sentinel condition reflecting systemic health. Its prevalence increases with age, yet it is hardly an inevitable consequence of aging. Rather, it serves as a clinical clue that vascular, metabolic, or endocrine pathways may be compromised. A man presenting with ED may, in fact, be presenting with early cardiovascular disease. For clinicians, this makes ED both a quality-of-life issue and a diagnostic opportunity.
The advent of phosphodiesterase type 5 (PDE5) inhibitors fundamentally altered the therapeutic landscape. Before sildenafil appeared in the late 1990s, treatment often involved vacuum devices, intra-cavernosal injections, or penile implants. While effective, these methods carried stigma and were hardly user-friendly. Oral PDE5 inhibitors brought simplicity, rapid onset, and — perhaps most importantly — discretion.
But with four agents approved worldwide (sildenafil, tadalafil, vardenafil, avanafil) and dozens of systematic reviews published, the clinical question persists: which agent is best for which patient? An umbrella review of systematic reviews attempted to synthesize this evidence, and it is this synthesis that we explore here.
Mechanism of Action: Sustaining the Signal
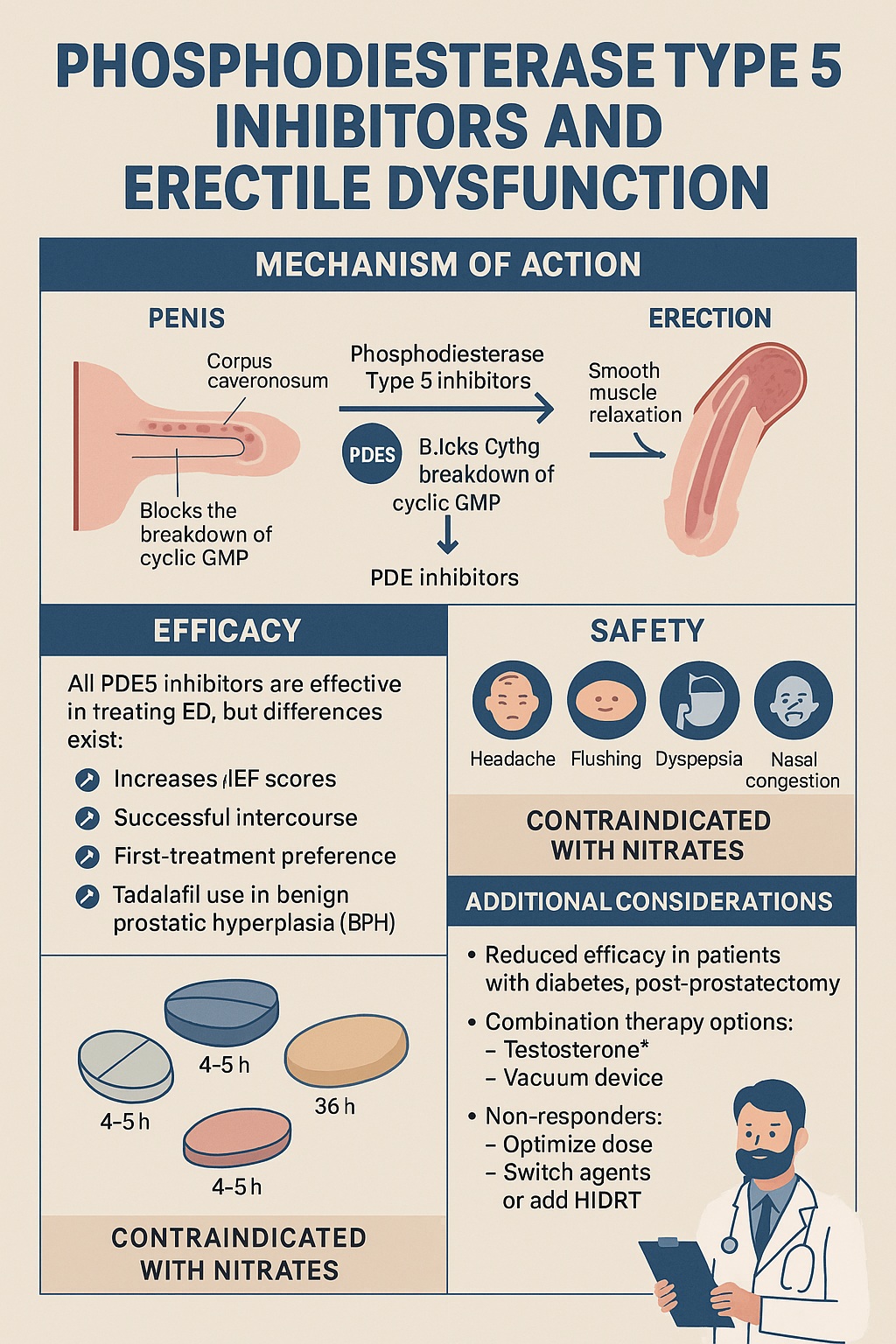
The physiology of penile erection is exquisitely orchestrated. During sexual arousal, nitric oxide (NO) is released from parasympathetic nerve terminals and endothelial cells in the corpus cavernosum. NO activates guanylate cyclase, which catalyzes the conversion of GTP to cyclic GMP (cGMP). Elevated cGMP triggers smooth muscle relaxation, dilates penile arteries, and allows cavernosal tissue to fill with blood.
The enzyme PDE5 degrades cGMP, effectively “turning off” the erection. By selectively inhibiting PDE5, these drugs prolong cGMP’s presence, allowing the erection to last long enough for satisfactory intercourse. It is worth emphasizing that PDE5 inhibitors do not create sexual desire nor induce spontaneous erections; rather, they potentiate the body’s natural response to arousal.
Subtle pharmacokinetic differences separate the molecules:
- Sildenafil: Onset in 30–60 minutes, half-life about 4 hours, absorption delayed by fatty meals.
- Tadalafil: Onset in 30 minutes, half-life 17–36 hours, unaffected by food, enabling once-daily or “weekend pill” use.
- Vardenafil: Similar to sildenafil but slightly faster onset and more potent at equivalent doses.
- Avanafil: Newest, with rapid onset (as little as 15 minutes) and fewer visual disturbances.
These distinctions, while minor in pharmacological terms, often influence patient preferences dramatically.
Efficacy in the General Population
Large-scale analyses converge on a reassuring truth: all PDE5 inhibitors are significantly more effective than placebo. The International Index of Erectile Function (IIEF), Sexual Encounter Profile (SEP), and Global Assessment Questions (GAQ) consistently show marked improvement. Yet differences emerge when comparing regimens.
Sildenafil, the archetype, remains the most extensively studied and the standard comparator in clinical trials. At 50–100 mg, it improves successful intercourse rates by 60–80%, compared with about 20–30% with placebo. Interestingly, even 25 mg shows substantial benefit, suggesting a therapeutic window at lower doses for men sensitive to side effects.
Tadalafil’s endurance advantage cannot be overstated. Its long half-life allows sexual activity over a 24–36-hour window, reducing the need for precise timing. Daily low-dose regimens (2.5–5 mg) have been especially effective, providing not only erectile improvement but also relief of lower urinary tract symptoms due to benign prostatic hyperplasia (BPH).
Network meta-analyses, which pool indirect comparisons, suggest modest differences: tadalafil daily may edge ahead in patient satisfaction, sildenafil remains first-line for occasional use, and avanafil provides a rapid option. Yet because head-to-head randomized trials are scarce, these rankings should be interpreted with caution.
Efficacy in Specific Patient Populations
While general efficacy is clear, ED is rarely “pure.” It is often secondary to chronic disease, and response rates vary across subgroups.
Diabetes Mellitus
Diabetic men have endothelial dysfunction, neuropathy, and reduced nitric oxide bioavailability — a triple assault on erectile pathways. PDE5 inhibitors remain effective but with lower response rates (around 50–60% compared to 70–80% in non-diabetics). Among the agents, vardenafil and sildenafil show the strongest performance in diabetic cohorts. Intensified lifestyle and glycemic control amplify their benefits.
Post-Prostatectomy Patients
Radical prostatectomy, even when nerve-sparing, disrupts neural and vascular pathways. PDE5 inhibitors are central to “penile rehabilitation,” aiming to preserve tissue oxygenation and prevent fibrosis. Daily tadalafil or sildenafil has been used in this context, with improved long-term function compared to on-demand regimens. Timing is debated: should therapy start immediately post-surgery, or once spontaneous erections fail? Current evidence leans toward early initiation.
Chronic Illness and Neurological Disorders
- Hypertension and renal disease: PDE5 inhibitors restore erectile function without significant blood pressure compromise, making them suitable even in complex polypharmacy regimens.
- Spinal cord injury and multiple sclerosis: Trials confirm benefits, though efficacy depends on lesion level and neurological preservation.
- Obstructive sleep apnea: By improving endothelial function, PDE5 inhibitors may help counteract ED associated with nocturnal hypoxia.
Psychogenic ED
A crucial distinction must be made: when ED is primarily psychogenic, PDE5 inhibitors often disappoint. In such cases, psychological interventions — cognitive behavioral therapy, couples counseling — are more effective. Combining these with PDE5 inhibitors rarely adds benefit, reminding clinicians that not every dysfunction is solved by a pill.
Safety Profile: Lessons From Two Decades
The broad use of PDE5 inhibitors has generated vast safety data. Overall, they are among the safest cardiovascular-active drugs available.
Common Adverse Events
- Headache, flushing, nasal congestion, dyspepsia: predictable from systemic vasodilation, usually mild and transient.
- Visual disturbances: linked to PDE6 inhibition, most common with sildenafil.
- Myalgia and back pain: more frequent with tadalafil, due to PDE11 inhibition.
These side effects are generally dose-dependent and diminish with repeated use.
Serious Safety Concerns
- Cardiovascular events: Initial anxieties about myocardial infarction risk have largely been dispelled. Meta-analyses show no increase compared with placebo, provided nitrates are not co-administered.
- Priapism: Rare, but requires patient education. Most cases involve misuse or combination with other erectogenic agents.
- Hearing loss and retinal ischemia: Extremely rare, with uncertain causality.
The most important safety message remains clear: never combine PDE5 inhibitors with nitrates. The resulting hypotension can be catastrophic.
Dose and Discontinuation
High-dose sildenafil (100 mg) yields the highest discontinuation rates due to side effects. In contrast, low-dose regimens maintain excellent efficacy with fewer withdrawals. Patient education about correct timing (e.g., avoiding fatty meals with sildenafil) prevents many false “non-responder” labels.
Combination Therapies: Beyond Monotherapy
Despite their success, PDE5 inhibitors fail in 20–40% of patients. Combination strategies are therefore attracting interest.
- Testosterone supplementation: In hypogonadal men, restoring testosterone levels enhances PDE5 inhibitor responsiveness. This combination is supported by both physiological rationale and clinical trials.
- Acupuncture: Trials in East Asia suggest synergistic effects with sildenafil, though placebo effects are difficult to exclude.
- Chinese herbal medicine: Combining tadalafil with traditional herbal formulations showed superior outcomes in some Chinese cohorts. Western replication, however, is limited.
- Mechanical adjuncts: Vacuum erection devices or low-intensity shockwave therapy used alongside PDE5 inhibitors appear promising in refractory ED.
It is important to note that not all combinations deliver. Adding α-blockers for men with LUTS provided no extra erectile benefit. Similarly, pairing PDE5 inhibitors with psychotherapy in psychogenic ED yields no additional gain compared to psychotherapy alone.
Non-Responders and Difficult Cases
Not every patient responds, even with correct dosing. Non-responders present one of the most challenging aspects of ED management.
Strategies include:
- Dose escalation, up to maximum tolerated.
- Switching agents, since individual pharmacodynamics vary.
- Adding testosterone in men with low serum levels.
- Adjunctive shockwave or regenerative therapies for severe vascular disease.
A frequent oversight is inadequate trial duration. Some men require multiple attempts — up to eight doses — before experiencing optimal efficacy. Patient counseling, therefore, is as crucial as pharmacology.
Special Considerations in Clinical Practice
Patient Preference
A striking finding across studies is that patient satisfaction often outweighs raw efficacy data. Some men prefer sildenafil for its familiarity, others tadalafil for spontaneity, and still others avanafil for discretion. A clinician’s task is less to dictate and more to guide patients toward a match that aligns with their lifestyle and expectations.
Comorbidities
Men with ED often harbor hypertension, diabetes, or metabolic syndrome. Treating ED with PDE5 inhibitors can indirectly encourage better adherence to lifestyle modification and cardiovascular prevention, as patients regain confidence and motivation.
Psychological Impact
ED is associated with depression, anxiety, and reduced self-esteem. The psychological relief provided by PDE5 inhibitors may be as therapeutic as the physiological effect. This is why even “placebo responders” report substantial improvement — belief and confidence are powerful co-therapists.
Limitations of Evidence
The umbrella review highlighted methodological shortcomings that cannot be ignored.
- Indirect comparisons dominate. Without large-scale head-to-head RCTs, relative efficacy claims remain tentative.
- Industry sponsorship. Many trials are industry-funded, raising concerns of bias.
- Heterogeneity of outcomes. Different studies employ varied questionnaires and endpoints, complicating pooled analyses.
- Short trial durations. Most studies last weeks to months, leaving long-term comparative safety largely unknown.
Thus, while confidence in placebo superiority is unshakeable, confidence in drug-to-drug hierarchies is modest at best.
Future Directions
The horizon of ED management is widening. PDE5 inhibitors remain central, but research is probing beyond:
- Regenerative medicine: Stem cell and gene therapies aiming to restore vascular and neural integrity.
- Biologics: Growth factor or platelet-rich plasma injections seeking to regenerate cavernosal tissue.
- Personalized medicine: Pharmacogenomics may one day tailor PDE5 selection and dosing to individual metabolic and genetic profiles.
Until these arrive, optimizing PDE5 therapy — through correct dosing, education, and combination approaches — remains the pragmatic gold standard.
Conclusion
The story of PDE5 inhibitors is one of medical serendipity turned triumph. Originally investigated as cardiac drugs, they became the cornerstone of ED management, restoring function and dignity to millions.
All approved PDE5 inhibitors are effective. Their nuances — onset, duration, side effect profile — matter less than matching the right drug to the right man. Lower doses frequently balance efficacy with tolerability, and daily tadalafil offers unique advantages in both ED and urinary symptoms.
Non-responders, combination therapies, and complex comorbidities continue to challenge clinicians. But overall, the therapeutic class has achieved what few drugs do: transforming not just clinical outcomes but also cultural conversation.
In the end, PDE5 inhibitors do more than sustain erections. They sustain confidence, relationships, and, indirectly, cardiovascular awareness. That is a legacy beyond pharmacology.
FAQ
1. Which PDE5 inhibitor should be prescribed first?
Sildenafil remains the benchmark first-line agent due to its extensive data and affordability. However, tadalafil may be preferable for men seeking spontaneity or daily low-dose therapy.
2. Are PDE5 inhibitors safe for long-term use?
Yes. Long-term studies show stable safety profiles. The main cautions remain avoiding nitrate therapy and monitoring for rare adverse events.
3. What if PDE5 inhibitors do not work?
Check for correct use (timing, food interactions), optimize dose, consider switching agents, and evaluate testosterone levels. For persistent non-response, combination therapies or regenerative interventions may be explored.
