

High dose sildenafil citrate as a salvage therapy for severe erectile dysfunction
The objectives of this study were to evaluate the efficacy and tolerability of high dose sildenafil as a salvage therapy for patients refractory to the maximum recommended dose of sildenafil. Fifty four fully evaluated patients with chronic erectile failure (ED) who had previously failed to respond to a home trial of sildenafil (100 mg) with erections suitable for sexual intercourse were studied. Each man was treated at home with sildenafil at escalating doses of up to 200 mg until either maximal response or intolerable adverse effects occurred. Erectile function was quantified using the erectile function domain of the International Index of Erectile Function (IIEF) before treatment, with sildenafil 100 mg and with maximal dose of sildenafil and a global efficacy question after 4 weeks of treatment.
The mean age of the study group was 59.6±11.2 y. 13/54 (24%) had arteriogenic ED, 16/54 (30%) had mixed vasculogenic ED, 9/54 (17%) had cavernosal veno-occlusive dysfunction, 11/54 (20%) had post radical retropubic prostatectomy ED and 5/54 (9%) had psychogenic ED. 13/54 (24.1%) responded to sildenafil at a median maximal dose of 200 mg, 4/13 required 150 mg and 9/13 required 200 mg. 41/54 (76%) failed to respond to sildenafil. Mean IIEF question 3 and 4 scores were 1.5 and 1.4 at baseline, 2.2 and 1.9 with sildenafil 100 mg, 2.8 and 2.5 with sildenafil 150 mg and 3.0 and 2.9 with sildenafil 200 mg, respectively. After 4 weeks, treatment was regarded as having improved their erections by 37%, 46.3% and 68% of patients with sildenafil 100 mg, 150 mg and 200 mg, respectively. 34/54 (63%) reported adverse effects with maximal dose sildenafil comprising headache (19), facial flushing (32), dyspepsia (14), nasal congestion (11), dizziness (5) and visual disturbances (5). 4/13 (31%) responders refused to continue treatment due to adverse effects.
In conclusion, sildenafil at doses of up to 200 mg is an effective salvage therapy for 24.1% of previous sildenafil non-responders but is limited by a significantly higher incidence of adverse effects and a 31% treatment discontinuation rate.
Introduction
Erectile dysfunction (ED) is the inability to achieve and maintain an erection of sufficient rigidity for satisfactory sexual intercourse. 1 Community based epidemiological studies suggest that sexual dysfunction, particularly ED, is a common disorder in patients and is associated with reduced quality of life. 2,3,4,5
Sildenafil citrate (Viagra TM , Pfizer, UK), a potent, competitive phosphodiesterase type 5 iso-enzyme (PDE-5) inhibitor, is the first oral medication to demonstrate significant and reliable efficacy in most patients with ED. 6 Following activation of the nitric oxide/cGMP pathway by sexual arousal, inhibition of PDE-5 isoenzyme by sildenafil results in increased corporal levels of cGMP and an augmented penile erection. 7 Sildenafil appears effective in restoring erectile function and improving intercourse success rates in a wide range of patients, including those with hypertension, diabetes, spinal cord injury, other concomitant medical conditions, and in those patients taking a wide variety of concomitant medications. Its efficacy appears related to the extent and severity of ED, with significantly reduced efficacy demonstrated in patients with severe vasculogenic ED, diabetic ED and post radical prostatectomy ED. 6,8,9,11
Jarow et al reported a sildenafil response rate of 65%, significant improvement in quality of life and a 35% incidence of adverse effects. 9 Virag reported similar results with a 60% response rate and a 26.75% incidence of adverse effects. 10 McMahon et al reported a similar response rate of 67.5% but a higher incidence of adverse effects of 53.6%. 11 These authors report a similar efficacy rate but a higher incidence of adverse effects compared to that reported by the Sildenafil Study Group. 6
The maximum dose of sildenafil recommended by the manufacturer is 100 mg. A study was designed to prospectively review a group of patients with chronic ED, unresponsive to sildenafil 100 mg, who were treated in a home setting with doses of sildenafil in excess of the recommended maximum dose (150 mg and 200 mg). Treatment efficacy, safety and tolerance was evaluated using serial physician interviews and the patient self administered IIEF questionnaire.
Materials and methods
Fifty four fully evaluated patients with chronic ED who had previously failed to respond to a home trial of sildenafil (100 mg) with erections suitable for sexual intercourse were studied. All patients had received focussed sildenafil usage education and had been re-titrated to confirm their non-responder status. The mean number of sildenafil uses prior to enrolment in this study was 7 tablets (range 5–16). All patients had been previously assessed using a standardised protocol and the etiology of their ED determined. This protocol included a history and physical examination, determination of fasting lipids, glucose and free testosterone, vibratory penile biothesiometry and penile colour duplex Doppler ultrasonography (CDU) before and after intracavernous vasoactive drug challenge (20 mg alprostadil). Rigiscan nocturnal penile tumescence testing, dynamic infusion cavernosometry and cavernosography (DICC) and phallopharmacoangiography were performed where clinically indicated. Patients with unstable coronary artery disease, low output congestive cardiac failure, hypertension treated with three or more drugs, currently prescribed organic nitrate medication or those with any other contraindication to renewed sexual intercourse or sildenafil were excluded from the study.
Each man was treated at home with escalating doses of sildenafil citrate (100 mg, 150 mg and 200 mg) taken 1 hour before planned sexual activity until either maximal response or intolerable adverse effects occurred. The primary efficacy end point was the response to the questions 3 and 4 of the erectile function domain of the International Index of Erectile Function (IIEF) after a trial of each dose of sildenafil. The secondary efficacy end point was the response to the global assessment question ‘Has this treatment improved your erections?’ after 4 weeks of treatment.
Results were analysed using standard statistical analysis including descriptive statistics and Student’s t-test.
Results
Fifty four patients with chronic ED and a mean age of 59.6±11.2 y were enrolled in the study group. The etiology of ED was psychogenic in 5 patients (9%), arteriogenic in 13 patients (24%), cavernosal veno-occlusive dysfunction (CVOD) in 9 patients (17%), MVED in 16 patients (30%) and post radical retropubic prostatectomy ED in 11 patients (20%). The mean duration of ED was 16.6 months (range 4–32). Twenty four patients had diabetes mellitus, 27 had hypertension, 26 had dyslipidaemia and 20 smoked cigarettes. Two or more vascular risk factors were present in 46 patients (Table 1).
Erections of sufficient rigidity and duration for satisfactory sexual intercourse occurred in 13 patients (24.1%) at a median maximal dose of 200 mg. Four patients (7.4%) required 150 mg and comprised 2 patients with psychogenic ED and 2 patients with arteriogenic ED. The remaining 9 patients (16.7%) required 200 mg and comprised 2 patients with psychogenic ED, 3 patients with arteriogenic ED, 2 patients with cavernosal veno-occlusive dysfunction and 2 patients with post radical prostatectomy ED. Nine of the 13 patients (69%) who responded chose to continue therapy with sildenafil. Overall, high dose sildenafil was effective in 4 out of 5 patients (80%) with psychogenic ED and 9 out of 49 patients (18.4%) with organic ED (Table 2). Of the 11 patients with post radical prostatectomy ED, 2 patients had undergone a bilateral nerve sparing radical retro-pubic prostatectomy (NSRRP) and one had undergone a unilateral procedure and the remainder non-nerve sparing procedures. The mean interval between surgery and treatment was 5.2 months. High dose sildenafil was effective in 1 man treated with bilateral NSRRP and in 1 man treated with a unilateral NSRRP.
Mean responses to questions 3 and 4 of the IIEF erectile function domain, the primary end point, were 1.5 and 1.4 at baseline, 2.2 and 1.9 with sildenafil 100 mg, 2.8 and 2.5 with sildenafil 150 mg and 3.0 and 2.9 with sildenafil 200 mg. The mean score for Q3 and Q4 for sildenafil was statistically superior to baseline, overall, in all etiological groups and at all doses (P<0.001). The overall mean score for Q3 and Q4 for sildenafil 200 mg was statistically superior to sildenafil 100 mg (P<0.05) but not to sildenafil 150 mg. The mean score for Q3 and Q4 for sildenafil 200 mg was statistically superior to sildenafil 100 mg (P<0.05) for all etiological groups except post radical prostatectomy ED (Figures 1 and 2). The global assessment by patients whether treatment improved their erections, the secondary end point, was answered in the affirmative at week 4 by 37% on 100 mg, 46.3% on 150 mg and 68% on 200 mg (Figure 3). The incidence of affirmative responses was statistically superior at sildenafil 200 mg compared to 100 mg (P<0.05).
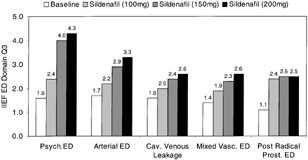
Response to IIEF erectile function domain Q3 at baseline, sildenafil 100 mg and sildenafil 200 mg.
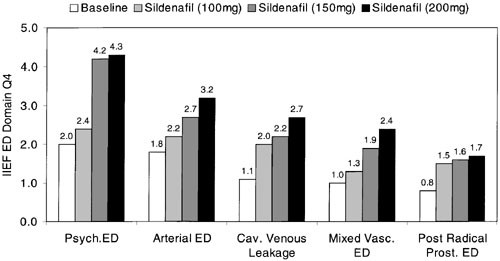
Response to IIEF erectile function domain Q4 at baseline, sildenafil 100 mg and sildenafil 200 mg.
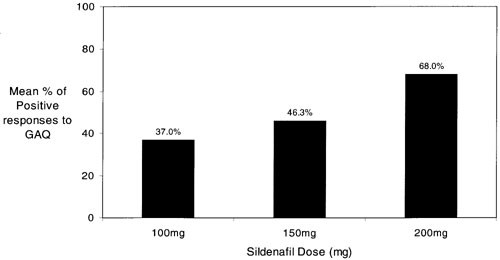
Mean responses to global assessment question (GAQ) with sildenafil 100 mg, 150 mg and 200 mg.
Thirty four patients (63%) reported adverse effects with maximal dose sildenafil. Eight of these 34 patients (23.5%) reported 1 adverse effect, 14 patients (41.2%) reported 2, 25 patients (29.4%) reported 3 and 2 patients (5.9%) reported 4 or more side effects. Facial flushing was reported by 32 patients (60%), headaches by 19 patients (35%), nasal congestion by 11 patients (20%), dyspepsia by 14 patients (26%), visual disturbances by 5 patients (5%) and dizziness by 5 patients (9%). Visual disturbances comprised transient light sensitivity (2), blue green visual aura (2) and blurred vision (1). Priapism was not reported. No cardiovascular adverse effects were reported within 24 h of taking sildenafil. One patient suffered an acute sub-endocardial myocardial infarction 5 days after last sildenafil use. A subsequent coronary angiogram demonstrated single vessel coronary artery disease involving the left main coronary artery. Two patients experienced exercise related angina pectoris. Neither experienced angina during sexual activity and the time interval between last sildenafil use and onset of angina pectoris was 4 and 9 days, respectively. Both had ST segment depression during exercise stress testing suggestive of coronary artery disease. None of these 3 patients had a prior history of coronary artery disease but all had significant multiple vascular risk factors.
The severity of adverse effects were assessed as mild in 51.2%, moderate in 31.4% and severe in 17.4% of sufferers (Table 3). Sildenafil responders reported a similar incidence and severity of adverse effects (61.5%) to non-responders (63.4%). Four (31.0%) of the sildenafil responders were not prepared to continue treatment with sildenafil due to intolerable adverse effects which included dyspepsia (3), facial flushing (4), headaches (3) and dizziness (1). Three of these 4 patients chose further treatment with intracavernous injection (ICI) and one underwent implantation of an inflatable penile prosthesis.
Discussion
The recognition that blood flow into the corpora cavernosa is regulated by vascular smooth muscle tone and that this tone can be pharmacologically altered with a variety of agents is regarded as one of the most significant advances in the treatment of ED. Initial therapy for ED should ideally be determined by etiology but also evidence based, depending on factors such as treatment efficacy, adverse effects, patient and partner acceptance, psychological effect, reversibility and cost. The ideal treatment for ED must be simple to take, non-invasive, non-painful, have a high success rate and cause few minor side effects. 12 Of the treatment options currently available, sildenafil most closely fulfils these criteria. The majority of ED sufferers currently choose oral therapy as a first line treatment and are prescribed sildenafil, the only PDE5 inhibitor currently available.
Response to sildenafil is reduced in chronic ED caused by either severe vasculogenic ED or post radical prostatectomy ED. Steers et al reported that only 55 and 59% of patients with severe ED achieved a response score of 4 or 5 to questions 3 and 4, respectively, of the IIEF inventory erectile function domain when treated with sildenafil 100 mg. Improved erections were reported by only 57% of patients with diabetes mellitus treated with sildenafil in a 3 month flexible dose study. 13 McMahon et al have reported that sildenafil is less effective in patients with CVOD as opposed to patients with arteriogenic ED. They demonstrated an inverse relationship between the severity of CVOD as determined by the DICC parameter, flow-to-maintain (FTM), and the response to sildenafil, as judged by patient scores to IIEF erectile function domain questions 3 and 4. They concluded that only patients with mild CVOD and a FTM ≤30 ml/min are likely to respond to sildenafil or combined sildenafil/ICI. 14 This is contrary to that reported by Shabsigh who suggested that sildenafil is effective in improving erectile function in patients with ED regardless of the etiology in a randomised placebo controlled study of 329 consecutive patients. 15 Shabsigh reported that although responses to questions 3 or 4 of the IIEF in patients treated with sildenafil were superior to placebo, responses did not differ in patients with organic, psychogenic or mixed ED.
The majority of the 30–35% of ED sufferers who fail to respond to the maximum recommended dose of sildenafil (100 mg), chose ICI therapy as second line therapy. Shabsigh et al reported that alprostadil therapy can be used effectively and safely in patients who fail initial therapy with sildenafil. In 67 patients who did not respond satisfactorily to sildenafil, alprostadil ICI resulted in significant improvement in questions 3 and 4 of the IIEF inventory erectile function domain in 60 (89.6%) and 57 (85.1%) patients, respectively. 16 Combined sildenafil and ICI therapy has been previously reported as effective salvage therapy for sildenafil non-responders. Twenty nine of 61 patients (47.5%) who failed to respond to sildenafil monotherapy, responded to combined therapy with sildenafil (100 mg) and Trimix ICI with an erection suitable for sexual intercourse. 14 Clearly ICI, despite lacking the obvious appeal of an oral medication, remains one of the major elements in the ED treatment armamentarium.
This study group comprised an unselected heterogenous population of chronic ED sufferers and included patients with psychogenic ED and organic ED of a predominantly vasculogenic aetiology. This study demonstrates that administration of sildenafil at doses of 150–200 mg results in sufficient rigidity to achieve vaginal intromission and complete satisfactory sexual intercourse in 24.1% of ED sufferers who had previously failed a trial of sildenafil 100 mg. This is contrary to the manufacturer sponsored pre-marketing studies, where the erectile response to a dose of 200 mg was not differentiable from 100 mg. 17 In this study, the response to sildenafil was independent of patient age and duration of ED but was highly dependent on etiology of ED. Rigidity sufficient for satisfactory sexual intercourse was reported by 80% of patients with psychogenic ED but only 18.4% of patients with organic ED. As has been reported previously, patients with CVOD appear less likely to respond to sildenafil as is the case with ICI treatment. Patients with CVOD, either as pure CVOD or as MVED, had significantly lower responses to sildenafil 200 mg than patients with arteriogenic ED (P<0.05). Clearly, our concepts about the etiology and mechanism of CVOD may need revision. CVOD is probably a multi-etiological condition involving not only degenerative cavernous myopathy, incompetence of the tunica albuginea or corporo-spongiosal shunts but also possibly disturbances of penile innervation or neurotransmitter release, failure in prostanoid synthesis or signal transduction via gap junctions, malfunctions of the enzymes nitric oxide synthase, adenylcyclase or guanylate cyclase or malfunction of the potassium channels. If this is in fact correct, it seems reasonable to assume that different etiologies of CVOD may respond to different treatments, that combination treatments may have a role and that our future management of patients with ED may re-focus on an evidence based etiological diagnosis approach in order to identify the most rational etiology specific treatment(s).
A failure to respond to sildenafil was common in patients with post RRP ED for prostate cancer. This parallels the experience of the Sildenafil Study Group who reported that only 43% of patients who had had RRP responded to sildenafil and suggested surgical damage to the cavernous nerves, with subsequent failure to activate the NO-cGMP pathway as the probable mechanism. 6 Our study group was unselected, relatively small and comprised a majority of patients who had undergone non-nerve sparing procedures. Improved results would be expected following a nerve sparing procedure. Lowentritt et al reported improved erections in 53% and improved capacity for sexual intercourse in 40% of patients taking sildenafil after nerve sparing RRP which was dependent on patient age, pathological stage and degree of nerve sparing surgical technique. 18 Hong et al suggested that the response to sildenafil was dependent upon the interval between nerve sparing RRP and reported that the treatment satisfaction increased to a peak at 60% 18–24 months after surgery. 19
Adverse effects were reported more frequently by participants in this study than by participants in the earlier studies although the adverse effect severity profile was similar. 6,8,9,20 Headaches, facial flushing, nasal congestion and dyspepsia remained the most common adverse effects. The higher incidence of reported adverse effects in this study clearly relates to the higher dose of sildenafil used. Adverse effects reflect the pharmacological action of sildenafil as a PDE-5 inhibitor and a weak PDE-6 inhibitor. Of particular interest is the fact that 31% of sildenafil responders were not prepared to continue treatment with sildenafil due to intolerable adverse effects. This contrasts significantly to that reported previously (2.6% and 9%). 6,11 This is, however, less than the reported alprostadil ICI drop-out rate of 37%. 21 As such, the role of high dose salvage therapy is limited by patient acceptance of a higher incidence of adverse effects.
This study reports a lack of major cardiovascular adverse effects associated with taking high dose sildenafil confirming the previously reported excellent safety profile of sildenafil. An increased risk of developing coronary artery disease and myocardial infarction in patients suffering ED is also demonstrated. An association between atherosclerotic coronary artery disease (CAD) and ED has been reported by several investigators. This is not surprising as the majority of patients with ED have vasculogenic ED due to atherosclerosis of the hypogastrico-cavernous axis. Furthermore, both clinical entities share the same risk factors including cigarette smoking, hypertension, hyperlipidaemia and diabetes mellitus. The incidence of acute myocardial infarction and cardiac death in this study exceeds that reported in the general community. 22
Several authors have suggested an increased incidence of silent myocardial ischaemia in patients with vasculogenic ED over the general community and identified vasculogenic ED as a possible independent risk factor for coronary artery disease. 23,24,25,26 Matsuzawa et al reported that 5 out of 20 patients with ED and no prior history of coronary artery disease, had exercise electrocardiogram changes suggestive of silent coronary artery disease. 24 Similarly, Kawanishi et al reported a 20.7% incidence of abnormal stress electrocardiograms in 58 patients with ED and no history of coronary artery disease. They reported abnormal stress electrocardiogram findings in 54.8% of patients with penile CDU evidence of vasculogenic ED as opposed to only 3.7% of patients with normal penile CDU. 25 Unfortunately the results of coronary angiography were not reported in either study so the high incidence of abnormal stress electrocardiogram findings reported almost certainly overstates the true incidence of silent myocardial ischaemia. Physicians must consider the cardiovascular status of ‘at risk’ patients with vasculogenic ED and significant vascular risk factors prior to initiating any treatment for ED including sildenafil. Sildenafil prescribing guidelines proposed by the ACC/AHA should be followed and ‘at risk’ patients may require cardiological assessment with exercise electrocardiography, stress echocardiography or persantin thallium stress testing. 27
Conclusion
Sildenafil is an effective treatment for ED in a broad cross-section of etiologies. As the first effective oral treatment for ED, sildenafil clearly appeals to those patients seeking initial treatment. This study demonstrates that 24.1% of ED sufferers who fail to respond to sildenafil at the manufacturer’s recommended maximum dose will respond to a higher dose of the drug. Their response is, however, limited by a significantly higher incidence of adverse effects. These side effects, despite being predominantly mild, are associated with a 31% treatment discontinuation rate.
